- Home
- Reconstruction of the MPFL after a Patellar Dislocation
Reconstruction of the MPFL after a Patellar Dislocation
SYMPTOMS
You have an unstable kneecap. You have fully dislocated it at least once. It is especially painful when freshly injured. Over time, especially if this happens several times, there is a very uncomfortable feeling of insecurity in the entire knee.
EXAMINATION
Upon examination, we find significant swelling of the knee joint and pain, especially on the inner side, when the injury is fresh. Sliding the knee to the outside is very uncomfortable for you (positive apprehension test). If the injury was some time ago, the typical gait pattern exists (unconsciously, weight is not put on the patella), minimal swelling, and increased sliding of the patella to the out-side, which can be more or less uncomfortable for you.
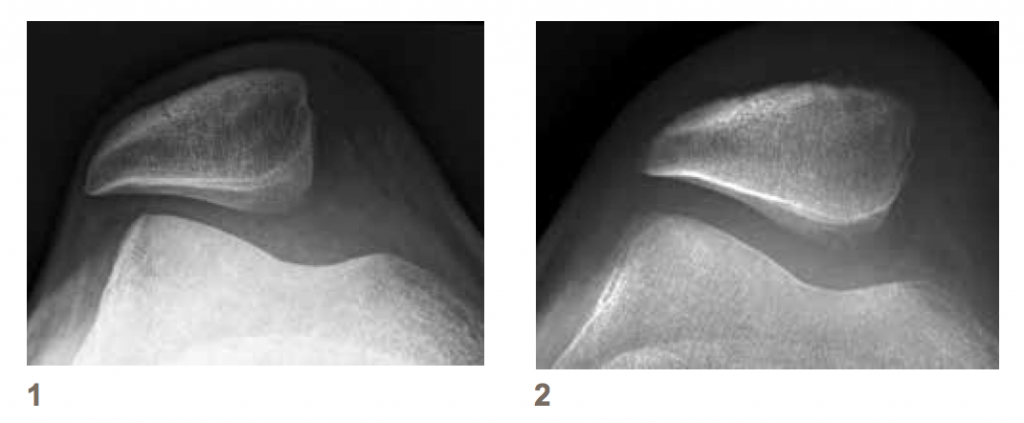
Images (X-ray, MRI, possibly CT) may show fresh cartilage/bone injuries on the kneecap itself. Consequences of injuries in the area of the medial patello-femoral ligament (MPFL), which should actually keep the kneecap on track, are also visible. Occasionally, more or less pronounced shape variations of the kneecap and the trochlea appears. This should possibly be taken into account in the treatment.
LEGEND
1 – X-ray of the right kneecap with a torn MPFL, the patella slides outwards
2 – X-ray of the right kneecap after an MPFL-Reconstruction with a centered patella
TREATMENT
Most cases can be treated conservatively. If there are no fresh cartilage/bone injuries and there is no relevant shape variation, you can try to stabilize the kneecap with physiotherapy. In case of persistent instability or accompanying injuries, we recommend the operative treatment and stabilization of the kneecap.
PROCEDURE
Stabilization of the kneecap with ligament reconstruction is recommended when there are fresh cartilage/bone injuries. It may be necessary to correct other existing injuries for reasons of instability, at the same time. A fresh carti-lage injury speaks for early intervention.
There are a large number of recommended surgical procedures for stabilizing the kneecap. We have had good experience with attaching a slender strip of the quadriceps tendon to the kneecap and diverting it towards the inside of the thigh bone (Fig. 3). We then attach this tendon strip at an anatomical location. We often combine this procedure with arthroscopy, and if necessary we open the joint to treat major cartilage damage.
Duration of the operation: depending on the complexity 45 mins. to 2 hours.
LEGEND
3 – Schematic representation of the stabilizing tendon strip on the inside
RISKS
You will be treated by experienced surgeons. And yet it is like flying: no surgery is without risk. The risks of this operation can be summarized as follows:
- Risk of infection: ~ 1%
- Likelihood that you will require a blood transfusion: ~ 0%
- Damage to relevant blood vessels: less than 1%
- Damage to relevant nerves: less than 1%
- Thrombosis/Embolism: ~ 1%
- Residual instability of the knee cap: ~ 10%
- Pain after injury and operation: ~ 20%
- Premature osteoarthritis after cartilage damage: ~ 20%
HOSPITAL STAY
The decisive factors are: minimal pain, minimal swelling, good mobility, and good wound conditions. After MPFL reconstruction, we recommend a knee brace that limits the knee flexion to 90 °, full weight-bearing is allowed with the full extention of the knee. You will usually be discharged within 3-5 days.
DISCHARGE
The stitches can be removed by your family doctor about 12 – 14 days after the operation. We will see you routinely after 6 weeks (with an X-ray), 3 and 6 months for check-ups in our out-patient clinic. Usually, you should be doing fine after 6 months and thus, we can then complete the treatment.
SPORT, what happens and when (after a basic MPFL-Reconstruction)?
Bicycle riding, on the street: after 8 – 10 weeks
Jogging: after 4 months
Tennis: after 6 months
Soccer and skiing: after 6 – 12 months
pdf for download: Patellar Dislocation