- Home
- Hallux rigidus
Hallux rigidus
DEFINITION/FORMATION
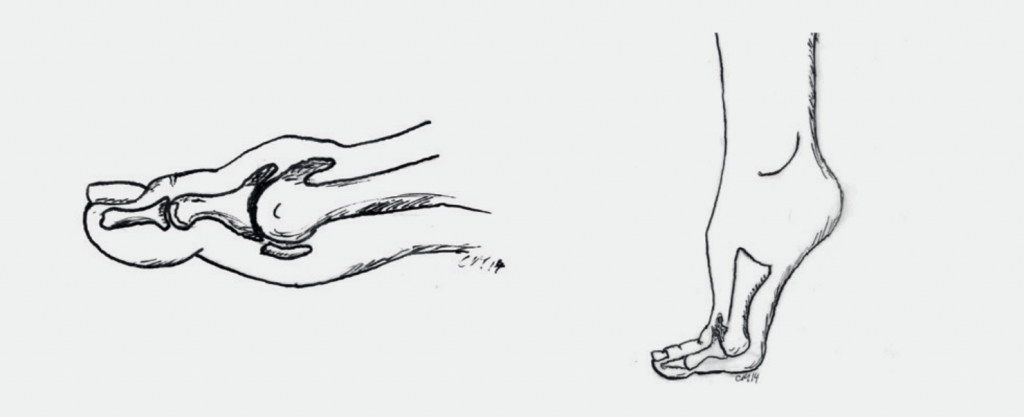
When movement in the big toe joint is painfully restricted, the cause is often the development of osteoarthritis of the joint, a so-called hallux rigidus. This is a degenerative change in the joint with partial destruction of the joint cartilage and development of bony spurs (osteophytes) at the edge of the joint surfaces. The change of the cartilage can lead to painful inflammation of the joint. The bony spurs and a too tight joint capsule can also reduce the range of motion. As the osteoarthritis progresses, the joint increasingly stiffens.
SYMPTOMS
Most patients complain of pain in the big toe joint area. Typically, these are start- up pains which intensify during/after exertion. Occasionally, pain while resting can also occur. The movement restrictions are not noticeable for most patients as they develop slowly. Forced movement of the big toe, on the other hand, causes pain because bone rubs against bone and the inflamed capsule is overstretched. In the final stage, once the joint becomes completely stiff, the pain will disappear. This can take many years though.
EXAMINATION
The examination often reveals a swollen joint with noticeable thickening of the bone and sometimes even redness. The range of motion is painfully restricted in all directions. The normal rolling of the foot while walking barefoot is often no longer possible.

The x-rays show the extent of the osteoarthritis (narrowing of the joint gap) and the bony spurs.
TREATMENT
A) Non Surgical
Depending on the severity of the symptoms, conservative treatments are suggested. These mainly focus on the mobilization and distraction of the toe through self- manipulation and/or physiotherapeutic support. Occasionally, a cortisone infiltration of the joint can be helpful. Wearing comfortable shoes with a rather firm sole usually causes less complaints because the movements in the arthrotic joint are restricted. We are cautious with prescribing insoles for stiff big toe joints. These insoles can change the gait pattern and cause pain in other places.
B) Surgical
If the osteoarthritis is already advanced or conservative treatments have been
unsuccessful, surgery is an appropriate treatment. There are various options:
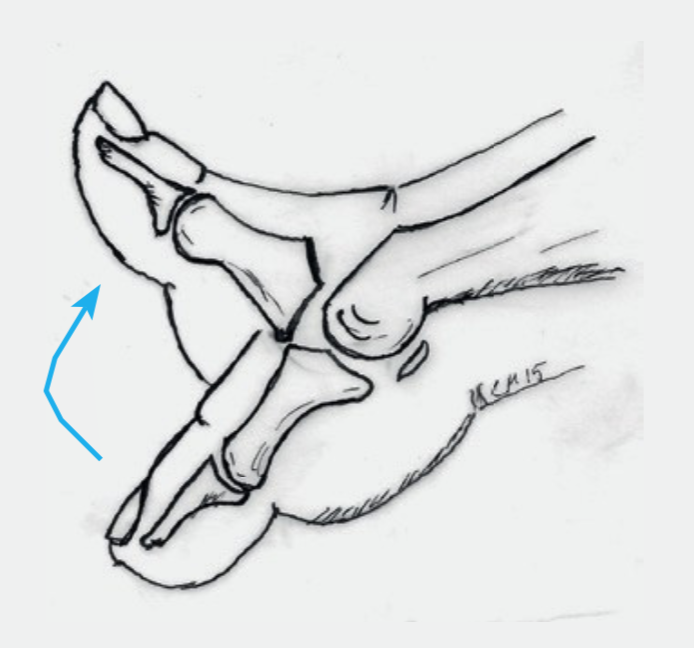
Cheilectomy: In most cases we perform a so-called cheilectomy (removal of the bone spurs) (Fig. 3). The excess bone is removed, and the joint is made slightly more flexible. However, the goal of the operation is not primarily to normalize range of motion, but to reduce the pain. After the operation full weight bearing is allowed. The amount of weight bearing depends on the subjective pain. It is vital that the toe movement is practiced from thestart.
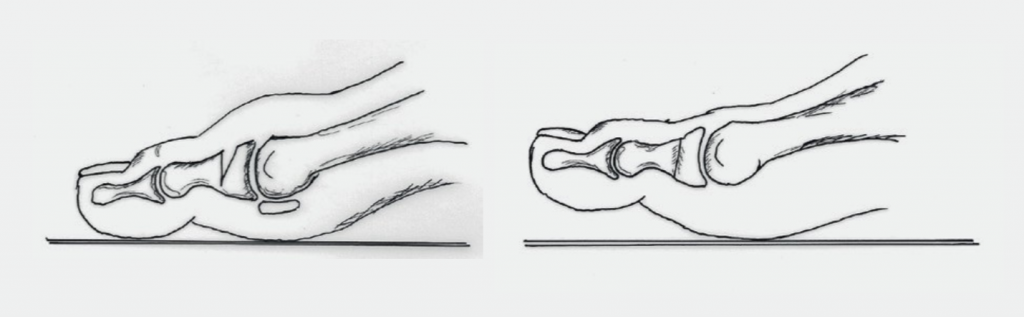
Osteotomy: If the toe has a pronounced restriction of movement mainly in one direction, a wedge of the bone can be removed. (Fig. 4). The bone is then fixed with a screw. The mobility gained in one direction (usually upwards) improves at the expense of the mobility in the other direction (usually downwards). After the operation full weight bearing is allowed as long as you are wearing a forefoot relief shoe (Fig. 6a). The amount of weight bearing depends on the subjective pain.
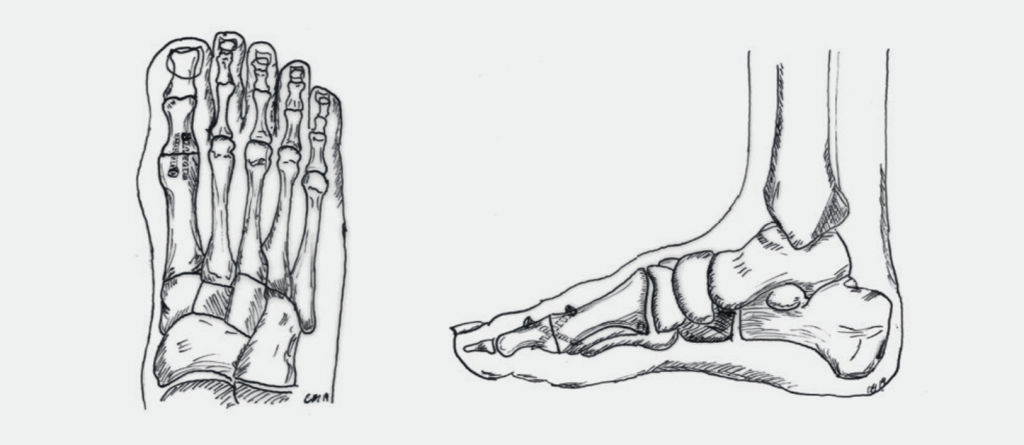
Arthrodesis:Inthecaseofsevereosteoarthritiswerecommendafusionofthe joint. Usually, a nearly complete spontaneous stiffness already exists in this situation. The difference is hardly noticeable to the patients after the operation, as even with a stiffened base joint, shoes with smaller heels can be worn and sport is not restricted. The fusion is done by using two screws or a small plate and screws. (Fig.5). You should not weight bear the foot for 6 weeks after the operation. Mobility and independence is possible using crutches and wearing a VACOpedes shoe (Fig.6b). After 6 weeks weight bearing can be increased, and normal shoes can be worn. In rare cases there need to be minor adjustments done to everyday shoes.
RISKS AND COMPLICATIONS
Complications and risks can occur during or after the operation, delaying the healing process or requiring another operation. Even though they are rare for foot operations, they can never be completely ruled out.
In summary, these are:
- Healing disorders
- Infections
- Vascular injuries, post-operative bleeding, hematoma, blood loss
- Nerve injury
- Non Union (lack of bone healing)
- Bothering implants (screws, plates)
- Thrombosis, embolism
- Residual symptoms
FOLLOW-UP TREATMENT
The surgery is only a part of the whole treatment. Follow-up treatment contributes significantly to its success. It is important that you know what you should be aware of and what you should possibly avoid.
Dressing and Wound Care
During the time in the hospital you will be shown how to take care of the wound. As long as the wound is not completely dry (wound secretions/blood), the dressing should be changed daily. Do not apply any ointments or powder directly to the surface of the wound until the stitches have been removed! Disinfection is not necessary. Always remove the entire dressing when changing. The new dressing must be dry and must not slip. Once the wound is dry, a normal bandage (quick bandage) is sufficient. An elastic bandage can protect and cushion the operated area. This will also reduce the swelling that is still present. If you are not sure whether everything is normal, you can contact your family doctor or contact us directly. The stitches can be removed about 2 weeks after the operation, this is usually done by the family doctor.
Swelling and Pain
After an operation, the affected foot is always more or less swollen. This swelling can recur for weeks (for up to 6 months). The most effective measure to prevent this is to elevate the leg. At home, the foot should be elevated often during the first few weeks. It also makes sense to move several times a day (walking, not as much standing) but only for a short time. It is time to elevate the leg if the foot is tense and starts to hurt again. It is important to know that the foot generally tends to swell after foot operations. This reaction is normal and disappears after 6 to 12 months. Pain in the operated foot can occur in the first few days and weeks after the operation despite these measures. However, to relieve the pain, you can take the pain medication prescribed to you.
Pressure
The permitted pressure on the foot depends on the operation performed. You received a special shoe to protect and simplify your mobility (Fig. 6). Depending on the operation performed, either partial weight bearing was recommended, or full weight bearing was allowed. In the first 2 weeks, partial weight bearing is usually recommended until the wound has healed.


Partial Weight Bearing
You can put about 25 kg of weight on your foot. This roughly corresponds with the weight of the leg and means that you always have to use crutches. Our physiotherapists will instruct you accordingly in order to be able to implement this correctly. It is important that you can use the stairs with the aid of crutches by yourself. It is also critical that the special shoe is worn consistently, and the crutches are used for the first 6 weeks.
Full Weight Bearing
As soon as the pain allows it, you may fully weight bear the foot. It is important that the special shoe is worn consistently throughout the first 6 weeks. The crutches are mainly used for security reasons and can slowly be omitted.
Personal Hygiene
As long as the stitches are still in the wound, i.e. usually in the first 2 weeks, the operated foot should be protected with a plastic bag. The easiest way is to pull the plastic bag over the special shoe. As soon as the stitches are removed, you can shower and bathe without further precautionary measures.
Thrombosis Prophylaxis
Thrombosis prophylaxis begins during the hospital stay. Depending on the operation, this prophylaxis must be continued. In most cases, we use the Fragmin 5000IE pre-filled syringes, which are injected by the patient themselves once a day. You will be instructed by our nursing staff during your stay.
How long you need the injections depends on the operation, the individual risks and is necessary until you can fully weight bear your foot and walk without crutches again, in about 6-8 weeks.
Work Ability
A rest period is crucial after an operation. In the first 2 weeks you should take care of yourself and not work. How long you will be unfit for work depends on the type of surgery as well as your stress profile. In most cases you and your employer should be able to temporarily find less stressful work. This enables early resumption of work.
The signed work absence that you will receive from us is a preliminary assessment. The certificate can be extended if you are not able to resume work after this time. If this is the case, report to your family doctor or to us.
However, you may take up your work again any time before the given date, if you feel capable to do so.
Driving a Car
At what point you can resume driving again depends on the kind of operation you had. You must refrain from driving as long as you cannot fully weight bear your foot or are still requiring crutches. How far thereafter your ability to drive is restored is up to you. In case of doubt or if you are unsure, we recommend to avoid driving.
Check-Ups
Your surgeon will require x-rays to be taken 6 weeks after the operation. The further procedure will then be determined. In most cases you will be able to wear your own shoes from then on. We recommend starting with shoes with a firm sole and soft upper leather.
Most activities can be resumed about 3 months after the operation. Sports activities should be increased slowly as not to provoke an overuse after a longer sport break.
pdf for download: Hallux Rigidus