- Home
- Info Center
- Frozen Shoulder / Adhaesive Capsulitias
Frozen Shoulder / Adhaesive Capsulitias
04.05.2020
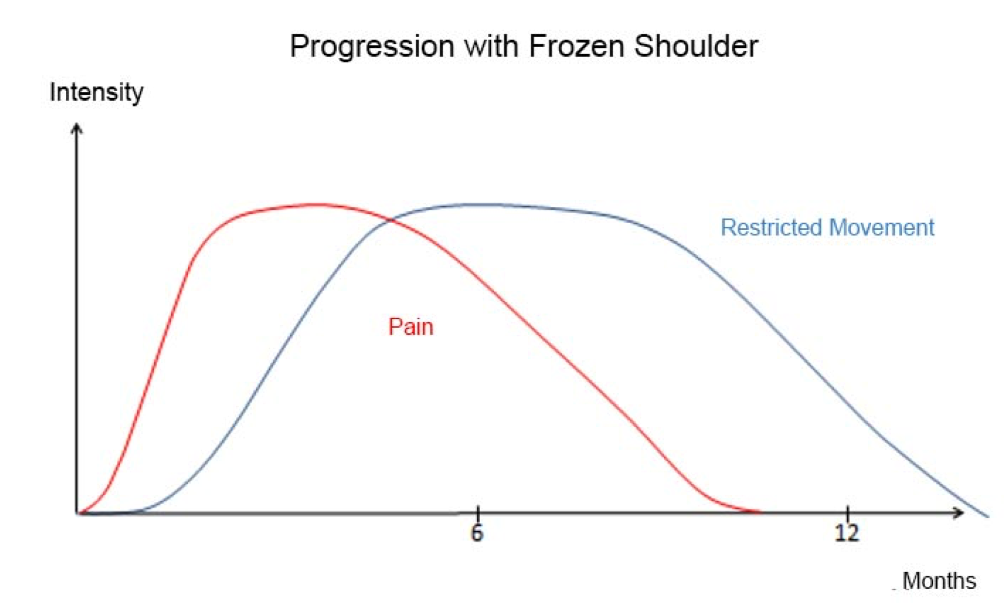
The actual frozen shoulder (FS) is a disease of the shoulder that is accompanied by pain and a temporary stiffening of the joint. It occurs without an actual trigger (primary FS) or can be triggered by minor accidents, general diseases or operations on the shoulder (secondary FS). In healthy people it occurs in 2-5%, diabetics have a risk of about 10%. The average age is 50 years. Women are more frequently affected than men. In 30% the disease occurs on both shoulders (independent of time). Recurrences are rare. The disease proceeds in three phases: The painful inflammatory phase, the stiffening phase and the relaxation phase.
Symptoms:
At the beginning of the disease you will only notice pain, which can increase significantly within a few weeks. Typical at first is a mobility-related pain, which then develops into a pain at rest. Especially at night you may experience the pain sharply. Your sleep will be severely disturbed by this. The pain can be triggered in all directions of movement and cannot be assigned to a specific movement. In these first weeks, the so-called inflammatory phase, it is very difficult to make a diagnosis, as no other symptoms can be detected.
After about 6 – 8 weeks following the onset of pain, you will then notice a gradual increase in restriction of mobility. Frequently, the external rotation of the shoulder is the first to be affected. The mobility can decrease so much that you are no longer able to stroke your head, put your hand down your neck or tie an apron behind your back. Only now, in the so-called stiffening phase, does the disease become apparent.
Usually the pain slowly subsides after about 4-6 months from the onset. From now on, the disease becomes bearable, although the restriction of movement remains much longer. After a certain period of time, you will slowly notice that your range of motion improves again. You are now in the relaxation phase.
Until you have completely overcome the disease, you must allow an average of 1 ½ years.
Examination
The diagnosis can be established primarily by a precise anamnesis (taking the medical history) and a clinical examination. However, it is important to rule out other causes of painful movement restriction of the shoulder (torn tendon, osteoarthritis, etc.). A normal x-ray is therefore advisable. Occasionally (especially at a later stage) indirect signs of FS can be detected by an MRI. However, an MRI is not the diagnostic tool of choice.
Treatment
There is no specific treatment for FS. Exercises to stop the joint from stiffening are painful and even counterproductive! Physiotherapy must be limited to the treatment of its accompanying symptoms (muscle tension around the shoulder blade).
The top priority is to avoid pain!
This also applies in everyday life. Drug therapy is often unsatisfactory because the pain does not respond well to common painkillers. Regular cooling of the shoulder is more likely to help. Cooling with lentil sachets is considered to be the most pleasant. If the pain is unbearable, infiltration (injection) of the shoulder with cortisone may be beneficial.
Only after the painful phase has subsided are you allowed to support the loosening of the joint with gentle stretching exercises. Only very rarely, if mobility does not return for several months although there is no longer any pain, an operative procedure may become necessary. Measures that shorten the duration of the disease have not yet been found.
But as a small consolation in conclusion: the prognosis of the disease is good. You do not have to expect any long-term consequences. All in all it “only” takes patience.