
WHAT IS A PLANTAR FASCIITIS, IS IT COMMON?
The most common cause of heel pain is plantar fasciitis, an overuse (irritation, inflammation, micro-damage) of the tendon plate in the arch of the foot. We call this tendon plate plantar fascia or plantar aponeurosis. Heel pain is very common, approximately every tenth person develops plantar fasciitis in the course of their life.
HOW DOES PLANTAR FASCIITIS DEVELOP?
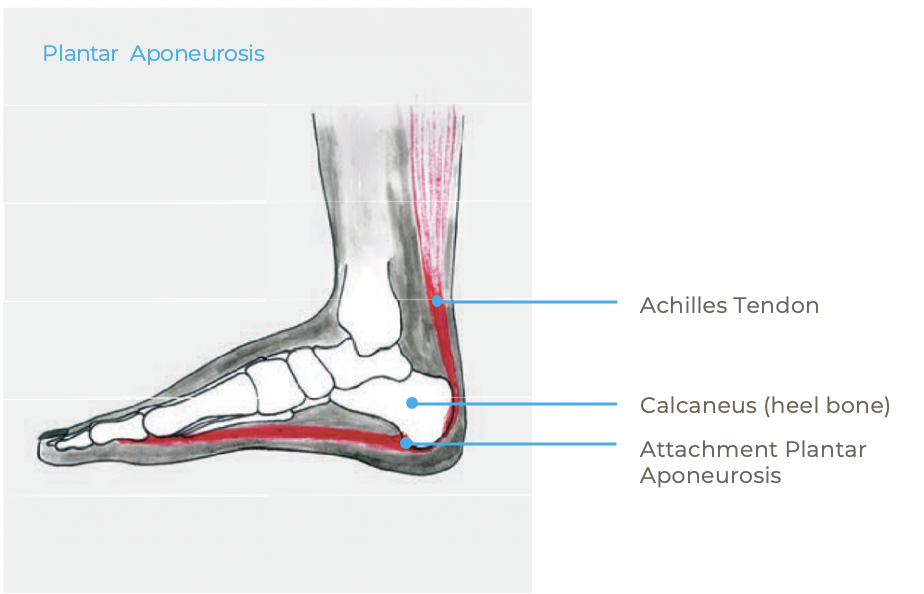
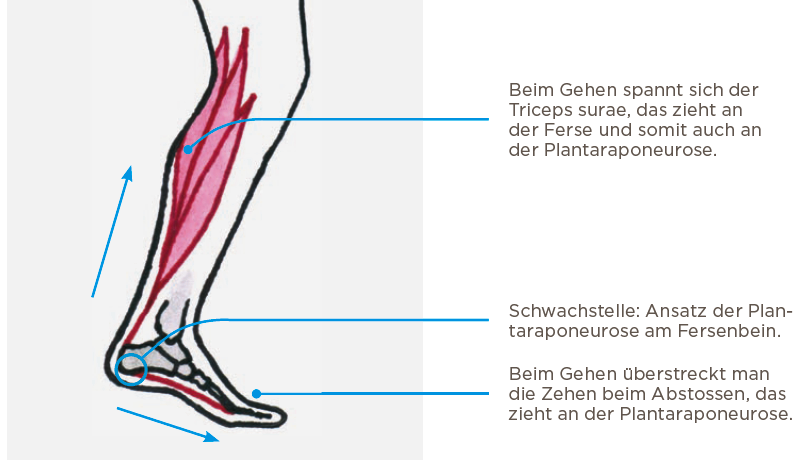
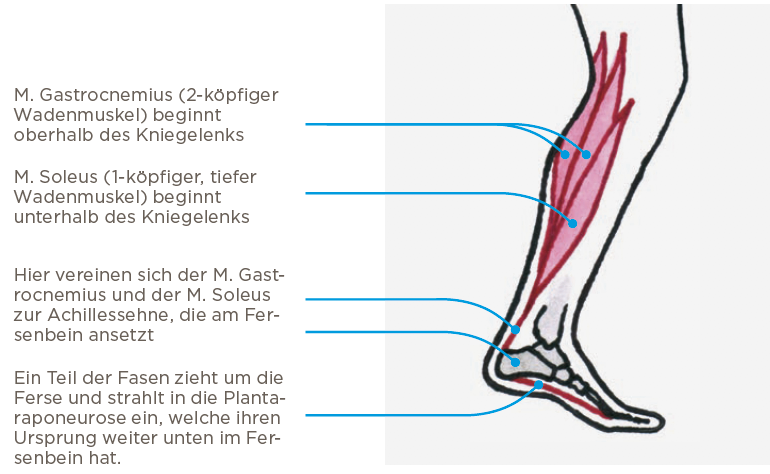
The plantar aponeurosis is attached to the heel bone and stretches all the way to the toes. It stabilizes the arch of the foot and is tense when standing and with every step taken. During the rejection phase, the plantar aponeurosis is strained by the overstretching of the toes. In addition, the calf muscles (triceps surae) pull on the plantar aponeurosis to transfer the pushing force to the foot. This leads to high traction forces on the plantar fascia. The weakest point is usually the insertion of the plantar fascia at the heel bone, which then canbe strained and inflamed as a result. The strain increases when going up the stairs or running.
ARE THERE RISK FACTORS?
Risk factors for the development of plantar fasciitis are predominantly a standing job, running and a body mass index (BMI) of over 30kg / m2. Certain foot shapes can also promote the problem, for examplea highly arched foot or a flat valgus foot. However, there is almost always a more or less pronounced shortening of the calf muscles and often also of the rear thigh muscles. This increases the burden of the plantar aponeurosis attachment on the heel.
WHY IS IT COMMONLY KNOWN AS “HEEL SPUR”?
Occasionally, an x-ray image shows a spur on the heel bone at the base of the plantar aponeurosis. This has led to the term “heel spur”, which is popularly used. However, this bone spur is not the cause of the pain. Only about half of the patients with heel pain have a heel spur and there are also people with a bone spur who have no pain at all.

WHAT DOES THE TREATMENT LOOK LIKE?
Therapy of heel pain is primarily non-surgical and consists of the following measures:
1. Symptomatic Treatment (in the first 2 weeks)
Resting. Pain-triggering activities should be avoided if possible so that the irritated structures can recover. Anti-inflammatory drugs or local anti-inflammatory measures (ultrasound etc.) can also help. However, the effect is often modest, since it is primarily a “mechanical” problem that cannot be solved “chemically”. Wearing heel wedges in your shoes for a short time also helps in the first days and weeks.
2. Treating the Cause (for months)
The most important thing is the reduction of tension and the pulling of the plantar aponeurosis. That is why a daily stretching of the shortened calf muscles and the plantar aponeurosis is the key to success. Since the shortening and the increased tension has developed over the years, these exercises must be carried out consistently for months. Some exercises are described in the appendix. To ensure correct implementation, physiotherapy can be prescribed. However, this does not change the fact that the exercises have to be carried out independently several times a day!
Physiotherapy is helpful in order to loosen and mobilize the hardened and tense muscles, tendons and fascia so that the stretching exercises can be carried out better.
3. Supportive Therapies
If the calf muscles are severely shortened, a night splint can be worn. There are ready made ones or it is possible to make one out of plaster. This should push the foot up at night or when no pressure is on it. The Strasburg Sock is a slightly less strong alternative that may be more comfortable to wear.
Focused shock waves promote blood circulation and tissue repair processes using mechanical stimuli. This treatment can be somewhat painful and does not help all patients equally well. Basic health insurance will not cover these costs.
Insoles make sense for certain foot shapes (buckling feet, hollow feet), as well as being a relief of the plantar fascia by providing soft bedding of the heel. The cost of the insoles is also not covered by the basic health insurance.
Insoles and shock wave therapy are complementary therapies and cannot replace daily exercises!
4. How to Avoid Recurrence
Even if the pain is no longer present after several months, the exercises learned should be continued about 3 times a week to prevent the pain from reoccurring.
WHAT ARE THE CHANCES OF SUCCESS?
90% of heel pain completely disappears under the therapy measures mentioned. However, this also takes 6-10 months even if the exercises are carried out consistently!
If the pain does not improve in six months despite the correct, repeated daily implementation of the exercises, a specialist assessment should be carried out again.